I’m too tired to make a story out of this, but here’s what happened today for anyone who is curious.
What one therapist giveth, another taketh away. This morning kicked off with another speech therapy session, and the SLP’s first order of business was to share the report from last week’s swallow test. It reiterated what I was told in-person when the test ended but included an additional note about a minor swallowing defect they noticed.* Since the swallow test did not show aspiration, and because additional testing was recommended, we can hold off on several of our upcoming appointments.
She instructed me to contact my GI, in case he wants to perform any testing himself. I suspect she’s never had a case like this before — she only graduated last year — or she’d know it’s technically the neurologist’s call on what to do next. But I got in touch with the GI and am waiting to hear back from him. Unfortunately, a few hours after messaging his office, the radiology report posted to my electronic health record. The radiologist documented things differently than the SLP who conducted the exam, writing the pill was lodged in my trachea.
This will complicate things from the GI’s perspective, and it also drove Crankenstein batty and probably temporarily inflamed ‘Niles.’** Fortunately, my speech therapist documented the note she received from her colleague, so the GI should also have access to that. My biggest concern is that I do not want to be scheduled for an endoscopy while having a feeling of tightness/heaviness in that part of my chest, because CRNAs are usually the airway attendants during endoscopy clinic procedures and that’s fine for routine twilight sedation during a pouchoscopy (or colonoscopy for you becoloned folks) but I want an actual anesthesiologist in the room if there’s a higher risk of emergency.
Next the SLP discussed breathing issues. During one of our exercises, I could only hold a particular noise she had me make for five seconds; a woman my age should be able to hold it for 10 to 15. We practiced some diaphragm expansion exercises and she told me to purchase a device called an EMST150 and bring it to our next appointment so she can adjust it and train me on how to use; it helps you improve the muscles needed for exhaling (or something like that). It’s different than a spirometer, a respiratory device I spent many months with while recovering from abdominal surgeries.
Once we were done, I met with a physical therapist who specializes in neurological conditions and she asked me a bunch of questions.^ The first thing I noticed was that she seemed like a young MAGA type, which stands out in an environment like a PT clinic because we were surrounded by lesbians who probably have Elizabeth Warren tote bags at home like I do. She seemed as uncertain of me as I was of her and I’m not sure if that’s because of my inexpressiveness, which she mentioned in her appointment summary, or if it was something else. Near the start of our discussion, she said that mine was a blanket referral, so even though fall prevention was our primary goal I could raise other concerns and we could possibly address those issues as well.
When I mentioned my underarm knot, a nagging problem for nearly three years now, she seemed disinterested. Something shifted later in the appointment and she interrupted herself to ask “Would you mind if I take a look at your underarm?” I can tell you the exact moment when she softened — she was telling me something like “I know you’re young and you’re used to doing things for yourself and being able to do them quickly. And we’re going to work to restore as much of that as we can, but one of the strategies you might have to try is expecting everything to take longer and planning activities accordingly.”
In other words, she wants me to accept my new limitations, so I replied “I guess in this line of work you’re part physical therapist, part psychologist.” Her neutral expression was replaced by a grin and she said yes, that’s often how she views her job. And then she asked about my underarm and found the knot immediately. Her first question was whether there’d been an ultrasound, because she wasn’t completely sure it was all muscle. I said imaging hadn’t turned up anything. She started yanking on my arm, folding it in different directions, and asking me questions. Then she asked if I would be willing to see a PT colleague of hers who specializes in orthopedics.
“She’s a shoulder expert and will know if this is related to your neck and your shoulder issues. She’ll be able to identify the muscles I’m having trouble with.” I agreed to a meeting and she told me it’s usually a long wait for an initial consult so she was going to pull some strings to get me in faster. True to her word, she got me on the books for Thursday. Being clueless about physical therapy, I had no sense of how the evaluation went. Mostly we did strength tests while I sat, things like “Extend your knee. Hold it. I’m going to try to push it down, do your best to stop me.” Then I walked in a line in front of her a few times, and we walked in circles around the gym while she timed me and trailed behind, observing my movement.
“How many more appointments are you scheduled for?” she asked when our time was up.
“Two,” I answered.
“We’re going to add another four to start with, and I’m going to request two with the shoulder specialist because it’s easier to cancel later than to schedule a followup if you need one.”
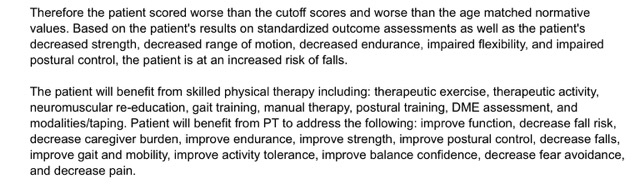
It was a Facts of Life sort of day, again taking the good (a break from speech therapy) with the bad (extra PT), and since we didn’t discuss the evaluation, I clicked on her visit note when I logged in to read the radiology report this evening. I assume some of this is boilerplate since, as she correctly noted elsewhere in her summary, I do not currently have a caregiver, but it could also mean “future caregiver burden” since most PD patients require assistance eventually.
Besides walking in circles with the PT, I covered familiar ground on the ride home, when my Lyft driver told me a very personal story about a recent trauma that derailed her life, and again later in the day when my work was interrupted by a buzzing phone.^^ Youngest Sister was sending messages about Tom, who she wants to toss off a bridge. That conversation went on, when time permitted, for the next couple hours, and it’s fair to say I also have ‘decreased endurance’ when it comes to my family.
* It was something I’d already told her was happening, which was that my swallow timing is ‘off’ sometimes, meaning I either swallow prematurely or it takes a couple tries. She said that’s common with PD.
** “You wouldn’t send a patient home with something lodged in their trachea,” Crankenstein said when I showed her the report. “You would summon an airway specialist because that’s an emergency. It’s also aspiration, which she notes you do not have.”
^ After the leg strength evaluation she asked if I’m willing to wear a leg brace or use a walking stick. When I took a moment to reply, she began filling the silence with a pitch about how a walking stick might enable me to walk faster or longer. She took pains not to say ‘cane,’ and I’d prefer a hiking stick if I needed assistance since others might assume I was just training for something, but I didn’t mention that to her. Since I’ve never heard of leg braces for Parkinson’s, I hoped it was a hypothetical as I replied “You’re the expert and I’ll try whatever you recommend, but my goal would be to delay the use of braces or mobility aids for as long as possible if that’s an option.”
^^ I’ve been told similar stories by girls and women, ranging from relatives and close friends to casual acquaintances and virtual strangers, countless times since I was in the eighth grade. Not because there’s anything special about me that puts people at ease, but because these particular traumas are so common that basically any woman who listens to other women hears about it constantly.